
From Awareness to Action:
Why Readiness Is the Missing Metric in Medical Education
How Throughline Strategy operationalizes the ALET Blueprint’s vision, turning the 8-stage readiness journey into a deployable measurement tool
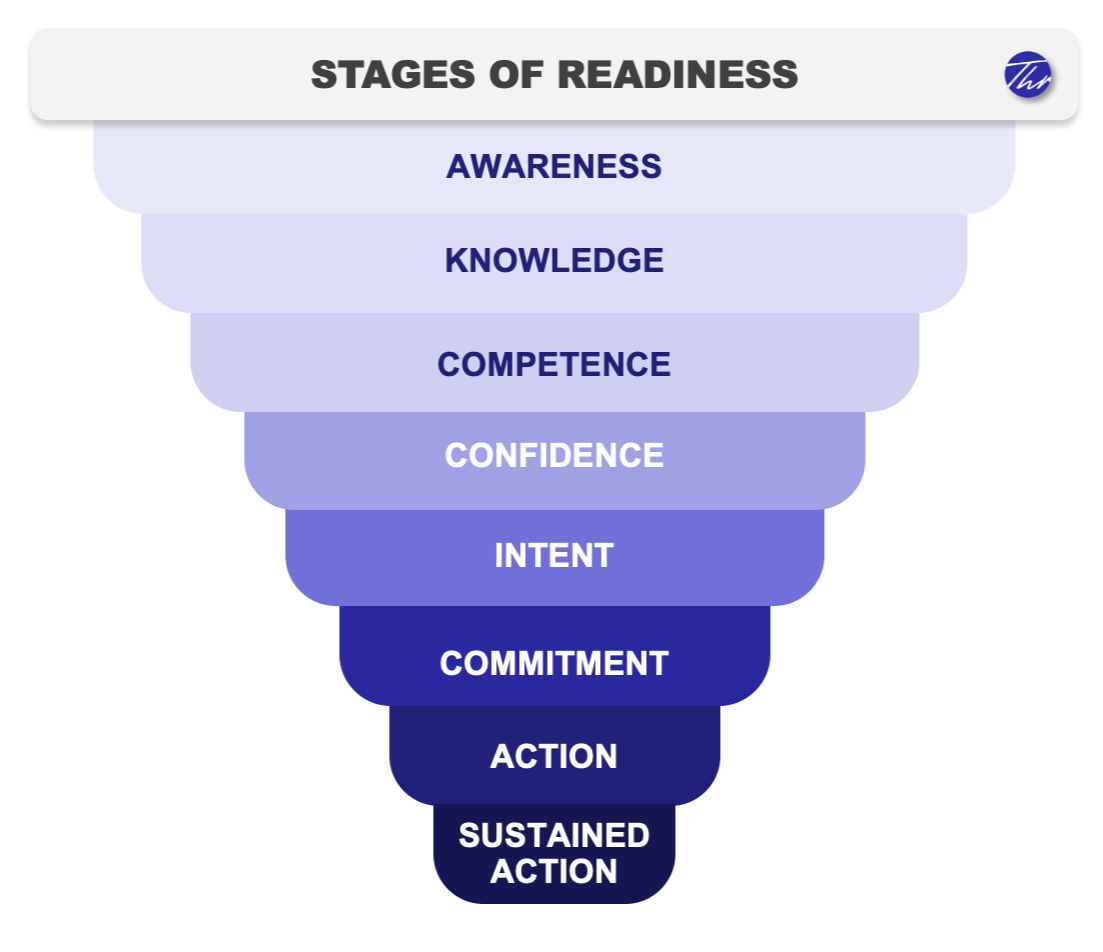
Figure 1. The Readiness to Act Framework: eight sequential stages from awareness to sustained action.
Visualization © Throughline Strategy. All rights reserved
The idea that behavior change happens in stages is not new. Since the early 1980s, researchers have known that people don't move from inaction to action in a single step; instead, they pass through a sequence of psychological states, each with their own logic and barriers. That insight gave us some of the most durable frameworks in behavior science, including the theory of planned behavior¹ and the social cognitive theory².
What medical education largely missed was how to operationalization it.
For decades, the field has assessed healthcare professional’s (HCP) learning needs the same way: surveys asking what they know, what they feel confident doing, and what they intend to change. The problem is that those data sit in separate siloes: knowledge here, confidence there, intent somewhere else, with no architecture connecting them into a picture of where an HCP actually stands in their journey toward practice change.³
In 2025, Paynter and colleagues put a number on the consequence: a $10 billion system achieving only 11% sustained behavior change! They went on to argue that the eight-stage journey from awareness to sustained action had long been treated as a passive checklist rather than an active architecture for designing education that actually changes behavior.⁴ To address this gap, they called for a methodological response and laid out their Applied Learning and Evidence Translation (ALET) Blueprint.
Throughline Strategy built the tool to operationalize the Readiness to Act framework to answer that call. If the stages are real, they should be measurable. If the levers that move HCPs between stages can be identified, they should inform content strategy. And if the same instrument is applied before and after an education program, movement between stages becomes a measurable outcome. It’s not a satisfaction score and not a knowledge quiz, but evidence of behavioral readiness shifting in the direction the program intended.
The core idea behind Readiness to Act
Readiness to Act applies the eight sequential stages established in behavioral change science, from awareness through knowledge, competence, confidence, intent, and commitment, to action and finally sustained action, as the backbone of a measurement and evaluation system. The stages are not arbitrary. They reflect a theoretically grounded sequence: in the same way that you cannot be confident doing something you are not yet competent at, you will not commit to a change you do not yet intend to make.⁴ ⁵ What this gives us that a standard needs assessment does not is a single, interpretable position for each HCP. Instead of scattered, disconnected scores, this gives us a location on a map. And like any good map, it tells you not just where someone is, but what it will take to move them toward a destination.
Where Throughline’s innovation begins
Knowing the theory is one thing. Using it to generate actionable insight at scale is another. Throughline takes an empirical approach that applies the Readiness to Act framework as a powerful tool that goes beyond an abstract concept.
Adaptive measurement
We design survey instruments that are calibrated to the specific clinical and behavioral landscape of each therapeutic area and HCP population. The questions that distinguish a committed rheumatologist from a merely confident one are not the same as those that make that distinction in oncology. Generic instruments produce generic findings. Ours are built to surface the distinctions that matter for a given program.
Driver modeling
Knowing where HCPs stand is only half the story. The strategic question is, what will move them? We use quantitative modeling to identify which attitudinal, motivational, and contextual variables are the strongest predictors of readiness advancement within a given audience. This turns our needs assessments into something a standard gap analysis cannot produce: a ranked, evidence-based list of the levers most likely to generate movement between stages. Medical education content strategy follows directly from that list.
Qualitative integration
Numbers tell you which levers matter, but they rarely tell you why. We embed structured qualitative inquiry into the framework to surface the reasoning, language, and lived experience behind the quantitative patterns. This is not a bolt-on option or afterthought, but rather is designed to validate and enrich driver analysis, and to give faculty the kind of verbatim insight that makes education feel relevant as opposed to generic.⁶
What previous approaches miss
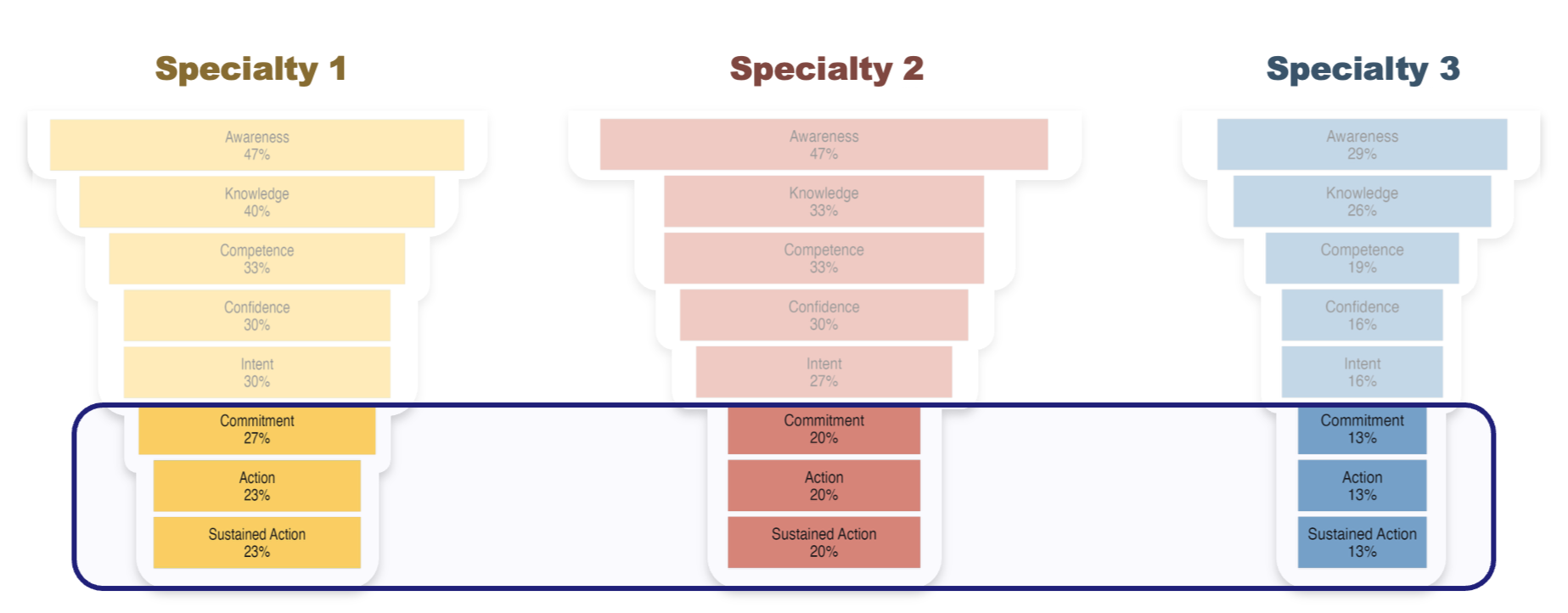
Figure 2. Readiness profiles differ meaningfully across specialties, a finding invisible to undifferentiated needs assessments. Each profile implies a distinct educational strategy.
A well-designed continuing medical education (CME) program can increase knowledge, which is measurable and important. But knowledge is only the second stage on an eight-stage scale.
The HCP who already knows the evidence but does not feel competent applying it to the complex patient in front of them does not need another didactic session. The one who is competent and confident but has not yet committed to changing their referral pattern needs something different still. Treating these two as the same audience, because both will score well on a knowledge quiz, is how education investment gets misallocated. Readiness to Act separates them. Stage movement, which refers to the proportion of HCPs advancing up the readiness scale, becomes the outcome metric. Not satisfaction. Not self-reported learning. Movement along the scale that predicts practice change.
This matters to Medical Affairs because it produces evidence that speaks the language of behavioral impact. It matters to program designers because it tells them not just what to teach, but who needs what, and in what order.
Where we are taking the Readiness to Act
Readiness to Act is a living methodology. We are currently developing the technical and empirical foundations for peer-reviewed publication, and expanding the framework's application across therapeutic areas, HCP populations, and program formats.
If you are designing a medical education program and want to understand where your audience actually stands, and what will move them, we want to connect with you.
References
Ajzen, Icek. "From intentions to actions: A theory of planned behavior." Action control: From cognition to behavior. Berlin, Heidelberg: Springer Berlin Heidelberg, 1985. 11-39.
Bandura, A. (1986). Social foundations of thought and action. Englewood Cliffs, NJ, 1986(23-28), 2.
Davis, D. A., Mazmanian, P. E., Fordis, M., Van Harrison, R., Thorpe, K. E., & Perrier, L. (2006). Accuracy of physician self-assessment compared with observed measures of competence: a systematic review. JAMA, 296(9), 1094–1102.
Paynter, C., et al. (2025). Stages of readiness for advance care planning: Systematic review and meta-analysis of prevalence rates and associated factors. White Paper
Burns, J. W., Glenn, B., Lofland, K., Bruehl, S., & Harden, R. N. (2005). Stages of change in readiness to adopt a self-management approach to chronic pain: the moderating role of early-treatment stage progression in predicting outcome. Pain, 115(3), 322–331.
Guetterman, T. C., Fetters, M. D., & Creswell, J. W. (2015). Integrating quantitative and qualitative results in health science mixed methods research through joint displays. Annals of Family Medicine, 13(6), 554–561